- About Us
- Ilizarov Technique
- Process
- Case Studies
Fractures
• Acute Fracture - Comminuted Fracture Distal Humerus - Compound Fracture & VAC • Nonunion - Proximal Tibia - Tibia - Distal Humerus • Malunion - Femur Bone Deformity
• Acute Correction
- LRS - Bilateral Tibia - LRS - Rotational Deformity Femur(with Shortening) - LRS - Oblique Plane Deformity Femur - Nailing • Ilizarov Correction - Proximal Tibia - Distal Femur • Hexapod Correction - Metaphyseal Dysplasia Bone Infection
• Infection - Femur • Infected Nonunion - Proximal Femur Joint Problems (Arthritis)
• Hip Replacement • Knee Replacement • Intra Articular Osteotomy • High Tibial Osteotomy (HTO) • Arthrolysis - Elbow • Ilizarov Hip Reconstruction - FAQs
- Testimonials



Deformity
Bones may become deformed for many reasons. These include congenital (from birth), developmental (from abnormal growth during childhood), and posttraumatic (from healing in a deformed position after a fracture).
Bones may be deformed in four ways: angulation (a bend in the bone), rotation or torsion (a twist in the bone), translation or displacement (a shift in the position of the bone after a fracture or osteotomy), or limb length discrepancy (a difference in the length of a bone compared with the other side).
Although each of the different types of bone deformities can exist on its own, it is very common to see combinations of two or more of these deformity components together.
There are various aspects involved in the process of deformity correction.
- How does the deformity develop?
- The "seat" of deformity i.e. the exact point from where the deformity is arising.
- Proper planning means more than half the work is done outside the operation room. The planning process for the deformity correction would include tracings, calculations, planning the osteotomy, placement of rings, pins etc. using various manual and computer aided tools.
- Execution of the plan keeping the minimally invasive principles in mind is another crucial step.
Corrective osteotomy (cutting the bone) requires either internal or external fixation to stabilize the broken bone.
Internal fixation is used in cases of acute correction (corrected at once, during surgery).
External fixation is used when it is preferable or safer to correct the deformity gradually to avoid stretch injury to soft tissues, such as nerves or blood vessels. Gradual correction of deformities is similar to limb lengthening. Certain instances where external fixator has distinct advantages over other methods:
- Bony bar in the epiphysis – hemi-epiphysiodesis would not be possible in such ascenario.
- Limb length discrepancy with or without deformity requires lengthening which is best performed using external fixator.
- Severe Valgus deformity - requires gradual correction to prevent any neurologic complication. The gradual correction is a virtue of external fixators.
One of the newer methods for gradual correction is using the Hexapod external fixator. This new powerful correction tool can simultaneously correct all four-deformity components utilizing the six-axis correction principle. It is a computer-aided correction where the software is used to guide the correction.
In children, gradual deformity correction can also be achieved by stapling one side of the growth plate called Hemi-epihysiodesis. This stops the growth of that side while the other side of the same growth plate continues to grow. Once the bone is straight, the staple can be removed to permit symmetric growth of the entire growth plate.
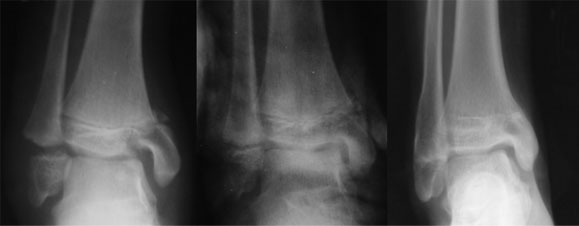
| How does the deformity develop |
| The xray picture shows one of the most common causes of deformity i.e. injury to the epiphysis(growth plate). As the growth plate heals it fuses and the growth arrests causing deformity. |
| There are various other causes of sectoral or complete growth arrests e.g. congenital or develeopmental growth plate defects, infection, hormonal imbalance etc. |
 |
| Planning |
Clinical picture and full length xray not only help in identifying the seat of deformity and any other deformities which may be masked, but also help in planning the kind and amount of correction, the overall biomechanics of the limb and also serve as a reference for future follow ups. Here in this particular patient the deformity is only in the proximal tibia (the leg bone close to knee), albeit on both the sides. |
 |